Every Tinnitus Treatment You Tried Failed You... And The Fix Is Simpler Than You Think.
See How To Finally Get Rid Of Tinnitus
You've done everything right. Tried every treatment, followed every recommendation. Hearing aids, medications, sound therapy. All of it keeps you dependent, not free. The same system that told you to "learn to live with it" makes billions every year on devices and therapies that were never designed to fix the real problem. A permanent solution doesn't generate repeat customers. That's why nobody showed you this. Watch the presentation below and see what they didn't want you to find.
The Explanation Your Doctor Never Gave You — And Why It Changes Everything
Most people get this far... and close the tab. They tell themselves they'll come back. They don't. And the ringing keeps going.
Finally Understand Why Nothing WorkedNo cost · No account required · Short Video
The Treatments You've Already Tried — And Why None Were Built to Solve the Real Problem
Every treatment you've tried was designed under the same foundational assumption: that tinnitus starts in the ear. The table below shows exactly why that assumption has kept millions of people trapped in the same cycle — and what would actually need to happen instead.
| Treatment | Why It Doesn't Stop the Ringing | What Would Need to Happen Instead |
|---|---|---|
| Hearing Aids Surface | Amplify external sounds — but never reach the internal signal being generated by the brain itself | RequiredAddress the neural signal directly, not the external sound competing with it |
| White Noise / Sound Masking Temporary | Covers the ringing — but the moment it stops, the brain resumes the signal at full intensity | RequiredInterrupt the neural loop at its source, not mask it on the surface |
| Most Supplements Misdirected | Formulated for ear health — not for the neural pathways where the signal is actually generated | RequiredAct directly on the central nervous system, where the signal is interpreted and sustained |
| Cognitive Behavioral Therapy Coping Only | Reduces emotional distress — but does not alter the neurological activity creating the sound | RequiredAddress both the perception and the origin of the signal, not just the reaction to it |
| Prescription Medications Indirect | Target anxiety or sleep — but leave the underlying neural disruption entirely untouched | RequiredInvestigate what is triggering abnormal signaling in the brain, not just its side effects |
Look at that list again — not as a catalog of options, but as a pattern. Every single approach was built on the same assumption. Every single one missed the same point. Which means every attempt you made wasn't a random failure. It was a predictable outcome of a framework that was never designed to address what's actually happening. And the longer that framework goes unchallenged, the more the cycle reinforces itself — quietly, without you realizing it's happening.
and that assumption is wrong...
what does that mean for everything you've tried so far — and everything you might try next?
Continue Your Research
You've been inside this cycle long enough. This is what it looks like from the outside — and why the exit was never where you were lookingFree presentation · Plain language · No account required
If Nothing Worked… The Problem May Be Bigger Than You Were Told
At this point, you've probably already reached the conclusion that most people with chronic tinnitus eventually reach:
- Not the medications.
- Not the sound therapies.
- Not the supplements or devices.
Because no matter what you try, the same thing keeps happening — the ringing never truly goes away. And after enough failed attempts, a more dangerous belief settles in: that this is permanent. That this is something you'll carry for the rest of your life.
But the most common response at this point isn't giving up. It's something quieter — and more costly. It's putting it aside. Telling yourself you'll look into it later. That you've already tried enough for now. And that decision — to wait, to postpone, to come back to it eventually — is itself part of the same cycle that has kept the problem unresolved. Not because you're not trying hard enough. Because every attempt so far has reinforced the wrong framework without you realizing it.
The longer tinnitus goes unaddressed at its actual source, the more embedded the signal becomes. What starts as occasional ringing becomes constant. What was manageable becomes something you structure your entire life around — avoiding restaurants, social gatherings, quiet rooms at night. The condition doesn't stay still while you're waiting for the right moment to address it. And every month spent inside a framework that was never built to solve the real problem is a month the cycle has to deepen. Most people don't recognize this until they look back and realize how much of their life the ringing has quietly taken over.
Recent neuroimaging studies have documented a significant anatomical overlap between the auditory processing regions involved in tinnitus and the areas associated with memory and cognitive function.[1,3] This is not a fringe hypothesis — it is an active and growing area of peer-reviewed research.
So If It's Not Your Ear… Here's Where the Sound Actually Begins
Every treatment you've tried was built on the assumption that tinnitus is an ear problem. But hearing doesn't happen in the ear — it happens in the brain. The ear converts sound waves into electrical signals. Perception, interpretation, and the persistence of sound are all neurological processes.
When normal auditory input becomes disrupted, the brain doesn't simply go quiet. It compensates. Instead of reducing activity, it increases sensitivity, amplifies internal signals, and tries to fill in what it believes is missing. At first, subtle. Over time, self-sustaining.
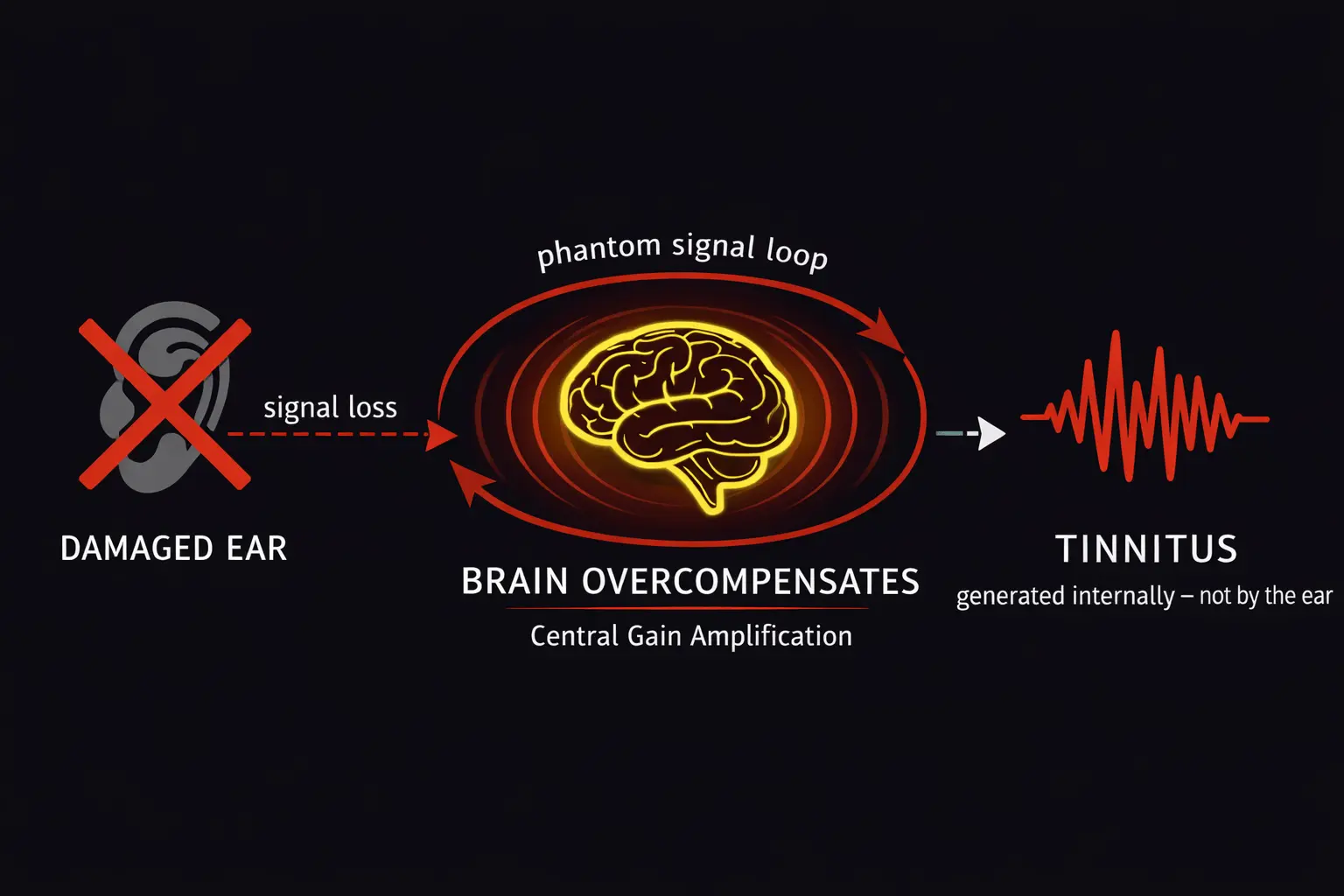
Once the compensatory signal becomes self-sustaining — a neurological loop — no external masking can stop it. Because the source is internal, continuous, and embedded in neural circuitry. This is what most treatments never address. And this is what recent research is beginning to examine directly.[1,4]
Watch Next
The signal isn't coming from where you've been treating it. This presentation shows exactly where it starts — and what that means for finally stopping itFree · No registration · Short Video
You Were Never Told This. And It Wasn't by Accident.
At this point, a reasonable question emerges: if the neurological evidence exists, why hasn't clinical practice changed to reflect it? Why are millions of people still being handed the same ineffective solutions — year after year — when researchers themselves are pointing to a completely different origin?
The answer isn't complicated. It's structural.
When a condition gets officially labeled as "chronic and incurable," two things happen simultaneously inside the medical and pharmaceutical ecosystem. First, research funding shifts away from finding a resolution — and toward optimizing management. Second, an entire industry worth over $2.3 billion gets built around keeping that condition under control, not eliminating it. Hearing device manufacturers collect an average of $4,000–$7,000 per patient in chronic management devices alone — devices that must be replaced, upgraded, and repurchased. And less than 3% of clinical trials conducted on tinnitus in the past two decades have focused on central neurological mechanisms. The rest tested peripheral approaches — the same ones that have consistently failed. Management, by definition, means one thing: you keep coming back.
This isn't a conspiracy. There's no single villain. But it is a system with deeply misaligned incentives — and you have been paying the price for it every single day. Every option inside that system generates recurring revenue. A permanent solution does not.
What has changed in recent years is not the system — it's the research happening outside of it. Independent neurological studies, conducted without the financial incentive to maintain the status quo, have begun examining tinnitus not as an ear condition to be managed, but as a brain-based signal disruption that may be addressable at its source. That research doesn't make headlines. It doesn't get advertised. But it exists — and it points in a very different direction than everything you've been offered so far.
You weren't failed by your own biology. You weren't failed by lack of effort or lack of trying. You were failed by a framework that was never designed to actually solve your problem.
See The Other Side of This Story
What independent researchers found when they stopped following the standard framework — and started asking different questionsFree · No registration · Short Video

"Some mornings I wake up and just lie there waiting for it to settle enough to get out of bed. My family tries to understand, but they can't really. I almost didn't watch this. I told myself I'd already seen everything. But something in the first few minutes stopped me from closing it. The explanation about what's actually happening in the brain was completely different from anything any doctor had ever told me. I finished the presentation and felt something I hadn't felt in years, that I was finally looking at the right problem. That alone changed how I approached everything that came next. For the first time in years I felt like my life was back. And in peace."

"The worst part for me has always been trying to sleep. When everything gets quiet at night, the hissing gets so loud it's almost unbearable. I worked through every option my doctor suggested — none of it made a real difference. What this presentation explained about why those things don't work was the first thing that made the whole experience make sense to me. I watched it twice. The second time I took notes. I hadn't done that with anything health-related in years, but this time I knew I was finally looking in the right direction. A few weeks later my wife noticed the difference before I even said anything."
"My tinnitus changes. Some days a high-pitched ring, other days more like static or cicadas. Three different specialists, same answer: learn to live with it. That never sat right with me. I've spent my whole career solving problems, not accepting them. After watching this I understood for the first time why everything I'd tried was built on the wrong premise. I followed through on what the presentation recommended. For the first time in a long time, I'm having conversations at dinner without asking anyone to repeat themselves. I forgot what that felt like."
Common Questions Before Watching
You Can Keep Trying to Silence the Noise… Or Finally Understand What's Causing It
This 15-minute presentation may be the first thing you've seen that addresses where the signal actually starts.
Watch The Presentation NowFree · No account · No obligation · Short Video
References
- De Ridder D, et al. "Tinnitus and the brain: a review of the neuroscience." Prog Brain Res. 2021;262:1–53.
- Bhatt JM, et al. "Tinnitus prevalence in the United States." JAMA Otolaryngol Head Neck Surg. 2016;142(10):959–965.
- Loughrey DG, et al. "Association of Age-Related Hearing Loss with Cognitive Function." JAMA Otolaryngol Head Neck Surg. 2018;144(2):115–126.
- Elgoyhen AB, et al. "Tinnitus: Perspectives from human neuroimaging." Nature Reviews Neuroscience. 2015;16(10):632–642.